1. Overview and Exposure Pathways
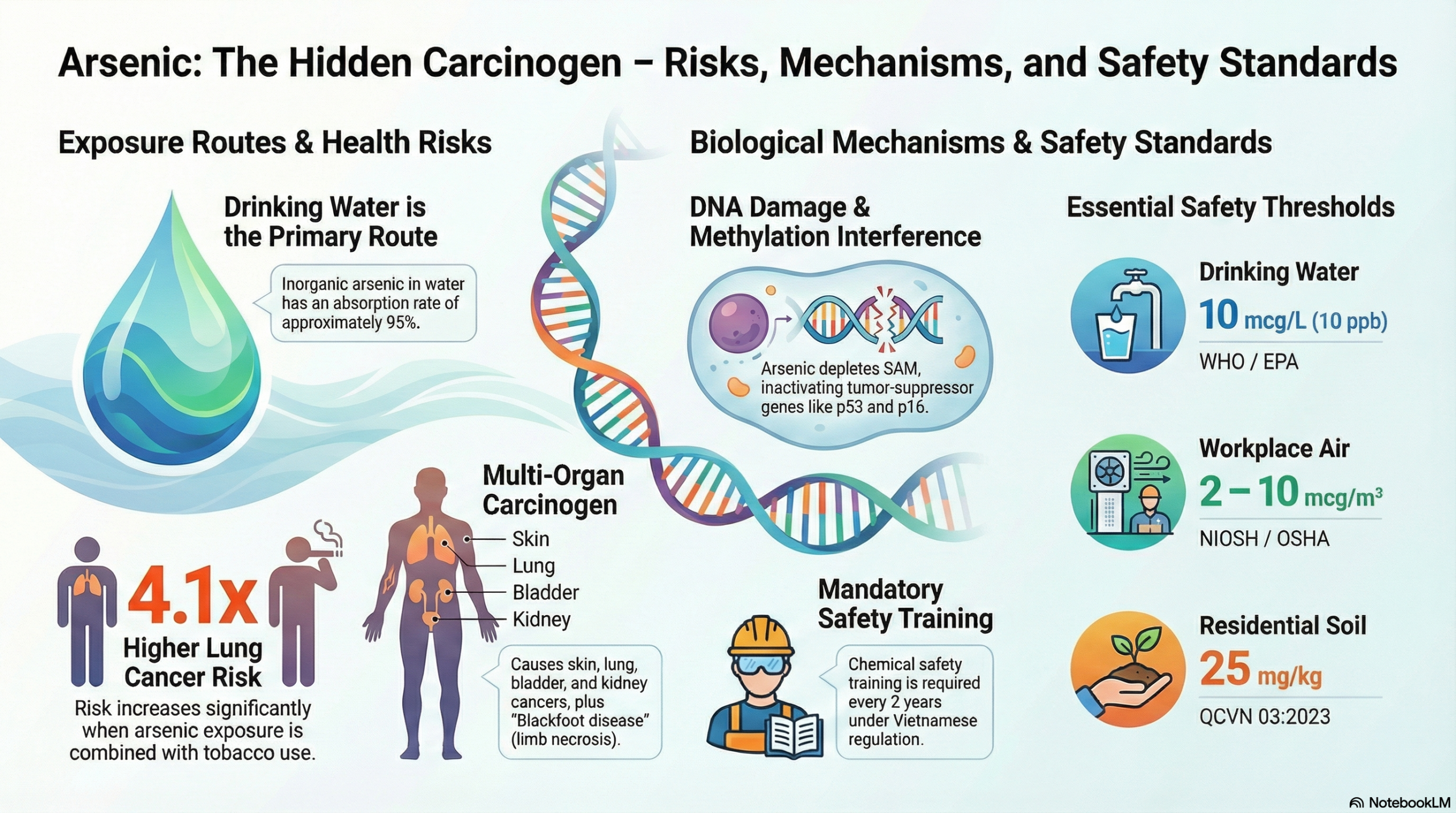
Arsenic (As) is a metalloid classified by IARC as a Group I carcinogen. Natural inorganic Arsenic contamination in drinking water remains the greatest threat (absorption rate ~95%). Other pathways include food (cereals, seafood), inhalation (metallurgical dust, coal combustion), and dermal contact. Chemically, trivalent Arsenic (AsIII) exhibits higher toxicity and cellular penetration capabilities compared to the pentavalent form (AsV).
2. Malignancies and Health Consequences
Chronic Arsenic exposure leads to the following disease burdens:
* Skin Cancer: The most common (Bowen’s disease, BCC, SqCC), typically appearing in non-sun-exposed areas after 10–30 years. Signs include palmar/plantar hyperkeratosis and pigmentary changes.
* Lung Cancer: The leading cause of mortality. The risk increases 4.1-fold when there is a synergy between Arsenic and tobacco smoke.
* Other Pathologies: Internal malignancies (bladder, kidney, liver); peripheral vascular disease (Blackfoot disease – gangrene of the extremities due to arteriosclerosis).
3. Biological Pathogenesis Mechanisms
Arsenic promotes tumor formation through indirect mechanisms:
* Methylation Imbalance: Arsenic metabolism consumes S-adenosylmethionine (SAM), causing the inactivation of tumor suppressor genes (p53, p16).
* Oxidative Stress: The generation of free radicals (ROS) causes structural damage and inhibits DNA repair processes.
* Epigenetic Modifications: Alterations in Histone structure and MicroRNA promote the epithelial-mesenchymal transition (EMT) to initiate cancer cell formation.
4. Medical Application: The As2O3 Paradox
Arsenic trioxide (As2O3) is an effective chemotherapeutic agent for Acute Promyelocytic Leukemia (APL) due to its mechanism of triggering apoptosis (programmed cell death). However, this therapy requires strict monitoring due to severe cardiovascular side effects and hepatotoxicity.
5. Technical Standards and Safety Management
To control risks, the following limit thresholds are established:
| Subjects | Threshold limit | Regulatory authority |
| Drinking Water | 10 mcg/L (10 ppb) | WHO, EPA, Việt Nam |
| Workplace Air | 2 – 10 mcg/m³ | NIOSH, OSHA |
| Agricultural/Residential Soil | 25 mg/kg | QCVN 03:2023/BTNMT |
| Industrial Soil | 200 mg/kg | QCVN 03:2023/BTNMT |
In Vietnam, according to Decree 113/2017/ND-CP, the production and trading of Arsenic must strictly comply with warehouse conditions, periodic safety training (every 2 years), and chemical incident response measures.
Summary
Chronic Arsenic exposure is a global public health challenge characterized by systemic toxicity and multi-organ carcinogenicity. Due to its latent nature and decadal lag effects, controlling Arsenic concentrations in water sources and occupational environments according to current standards (such as QCVN 03:2023) is the prerequisite solution. Furthermore, deeper research into epigenetic mechanisms not only supports early diagnosis but also opens prospects for targeted therapies, optimizing the management and reduction of the Arsenicosis disease burden in the future.
Center for Support & Continuing Education